Frozen Shoulder: Current Concepts & Concerns, and the Role of Arthroscopic Capsular Release
Frozen Shoulder, also known as Adhesive Capsulitis, is one of the most frustrating shoulder conditions—both for patients and clinicians. It leads to severe pain, significant stiffness, and functional limitation that can last months or even years. With evolving research and improved arthroscopic techniques, the understanding and management of Frozen Shoulder have changed dramatically.
What Exactly Is Frozen Shoulder? — Current Concept
Frozen Shoulder is now widely understood as a self-limiting inflammatory condition involving:
- Chronic inflammation of the joint capsule
- Thickening and contracture of the capsule
- Loss of elastic properties, especially in the rotator interval, coracohumeral ligament, and axillary pouch
- Progressive restriction of active and passive ROM
Updated Pathophysiology
Recent studies show that Frozen Shoulder behaves very similar to a fibrotic disorder, involving:
- Fibroblast proliferation
- Excess collagen deposition
- Capsular hypervascularity
- Cytokines like TGF-β driving fibrosis
This means it’s not merely “stiffness”—it’s an active disease process.
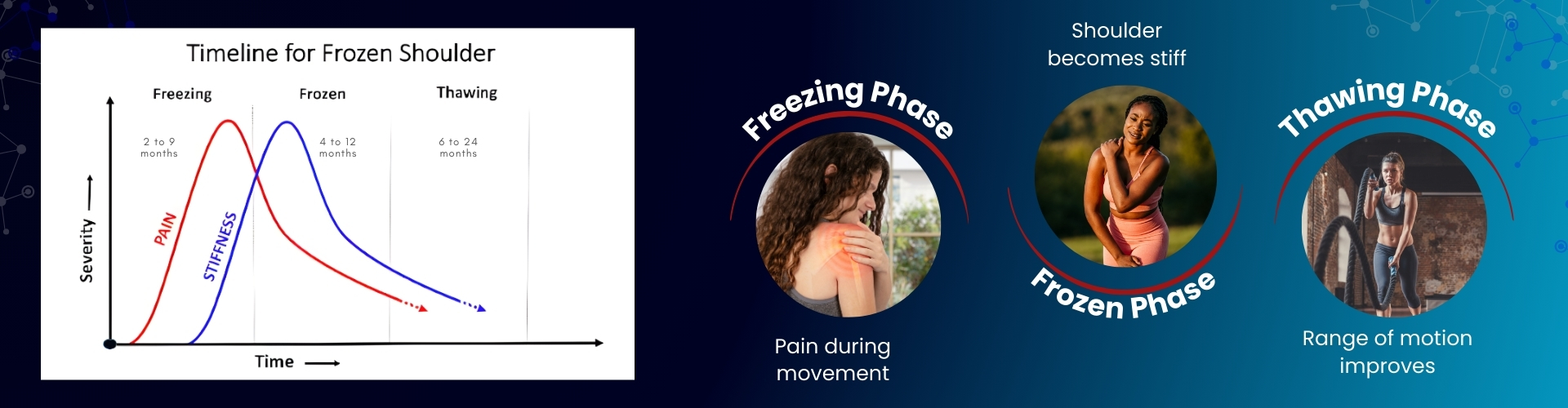
Stages of Frozen Shoulder (Current Clinical Understanding)
Treatment Options for Frozen Shoulder
| Treatment Category | Options | Purpose / Benefit |
|---|---|---|
| Medications |
|
Pain & inflammation control |
| Injections |
|
Reduces inflammation, improves early ROM |
| Pain Management | Suprascapular Nerve Block | Significant pain relief; helps physiotherapy |
| Physiotherapy |
|
Mainstay of treatment; improves ROM |
| Non-operative Procedures | Manipulation Under Anaesthesia (MUA) | For tough cases; may improve ROM rapidly but has risks |
| Surgical | Arthroscopic Capsular Release (ACR) | Gold standard for resistant cases; precise capsular release |
| Post-treatment Rehab |
|
Maintains gains & prevents re-stiffening |
Arthroscopic Capsular Release — The Game Changer
When conservative treatment fails after 3–6 months, Arthroscopic Capsular Release (ACR) has become the gold standard.
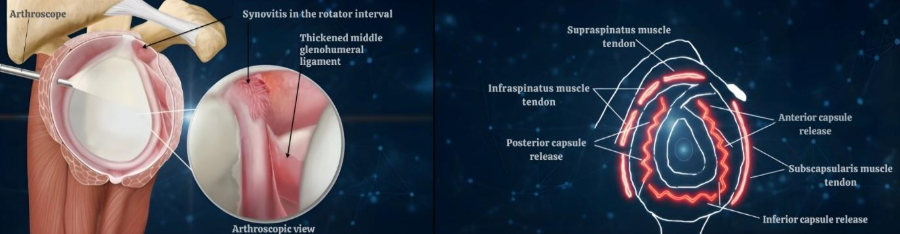
What Is Done in ACR?
A 360° release may include:
- Rotator interval release
- Coracohumeral ligament release
- Anterior and posterior capsule release
- Inferior capsular release (axillary pouch)
This technique frees the contracted capsule, restoring near-normal shoulder motion almost immediately.
Patient Selection: Who Benefits Most from ACR?
- Persistent stiffness > 3–6 months despite PT and injections
- Diabetic patients with resistant stiffness
- Post-traumatic or post-surgical stiffness
- Stage II (Frozen) adhesive capsulitis with capsular contracture
- Patients with occupational demands for early mobility
- Cases where MUA is contraindicated or has failed
Advantages of Arthroscopic Capsular Release:
- Immediate improvement in range of motion:
- Precise and controlled release:
- Safe and minimally invasive:
- Best option for diabetics:
- Addresses associated pathologies simultaneously
Physiotherapy becomes effective right after surgery.
Arthroscopy allows targeting exactly where the capsule is contracted.
Low complications when done by experienced surgeons.
Results are superior to MUA (Manipulation Under Anaesthesia) which carries higher risks of fracture or cuff tears.
Such as:
Post-Release Rehabilitation — Crucial for Success
ACR is only half the job; aggressive physiotherapy should start same day or next day.
Key rehab goals:
- Maintain the released capsule
- Control postoperative pain
- Gradually strengthen rotator cuff & scapular stabilizers
Takeaway Message
Frozen Shoulder is no longer seen as a simple condition that “gets better on its own.”
It is afibro-inflammatory capsular disorder that may take years to resolve, especially in high-risk groups.
Arthroscopic Capsular Releasestands out as an effective, safe, and reliable solution—restoring movement, reducing pain, and helping patients regain daily function much faster than conservative methods.
References
https://jassm.org/frozen-shoulder-release-ten-step-technique/